

| Online: | |
| Visits: | |
| Stories: |

| Story Views | |
| Now: | |
| Last Hour: | |
| Last 24 Hours: | |
| Total: | |
The lucky ones were vaporized: Hiroshima, Nagasaki, and genetics

I was alive when the two bombs, Little Boy and Fat Man, were dropped on Japan, but I was too young to know about it. Only years later did I know in some abstract sense what dropping the “A bomb” was all about. It was a merciful act, designed to end WWII before hundreds of thousands of soldiers on both sides were slaughtered or disarmed (literally), no?
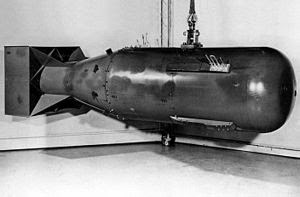 |
| Bombs away. Little Boy (wikipedia) |
I'm reading a new book Hiroshima Nagasaki, by Paul Ham. According to the author, by the time our testing was over and we were ready to deliver our babies, both the Allies and the Japanese knew that Japan was finished. The Nazis had just surrendered, having suffered but a fraction of what they deserved, and the Allies' attention could be turned full-bore on Japan. Pincers from China, Russia, the US and Britain were closing in on the besieged island Japanese. But if those suicidal maniacs (as we were told they were) decided to fight to the last samurai, countless good guys, as well as suicidal maniacs, would suffer. If we let the Japanese have a look at what we could do, then they'd surrender quickly and no battle for invasion would be needed.
To make sure they got the message, the Allies decided to give them a very close look, not at a bomb dropped in the harbor but the first directly on Hiroshima, not off-shore. The second was insurance. There were about 100,000 killed outright and 100,000 injured. There were hundreds of thousands who survived exposure to one (or in a few cases both) of the bombs, and of those who did not die of radiation sickness, life would never be the same. While some managed to have normal, or even happy lives, for many or most there was a huge lifelong trauma of radiation-related diseases, disfigurement, social ostracization, suicide, and other forms of misery. PTSD hadn't even been defined, but in some ways, the lucky ones were varporized.
MT readers may not know some of the biomedical aftermath and the way that these events not only ended a war but began a search for understanding of the biological effects of radiation exposure on humans. At war's end, the Atomic Bomb Casualty Commission (later renamed the Radiation Effects Rsearch Foundation, or RERF) was established to do research on the surviving victims. Their position when the bombs fell, shielding (e.g., in a house, out in the open), and resulting dose exposure were estimated for tens of thousands of bomb survivors. Their health was followed with regular examinations and so has been the health of their children in the nearly 70 years since the events.
Two leaders of the studies of these effects were the late Jim Neel and still-kicking Jack Schull. They were leading geneticists at the time (indeed, were among the founders of the American Society of Human Genetics). I was fortunate to be Jim's post-doc at Michigan and to have Jack on my PhD committee and as my department director in Houston for about 13 years. I was not directly involved in the RERF, but I did co-author with Jack a book-length report on radiation and cancer for a UN radiation agency. So while I've never been to Japan, I've followed some of what has gone on there, from a genetic point of view, for many years.
Why genetics?
Why would geneticists get involved in studies of A-bomb survivors? Wouldn't trauma surgeons, plastic surgeons and the like be the ones to be involved in the post-bomb medical studies? The answer takes us deep in to the nature of genetics and evolutionary theory of the time.
Before the war, it had been shown experimentally that atomic radiation was mutagenic. Whatever genes were, radiation could induce heritable changes in them. Radiation was one source, but we were exposed to others, such as cosmic radiation, chemicals and who knew what else. If mutations caused disease or deformity, then a species had to have a way to purge mutations from its populations if it were not to be mutated into extinction. Some theory held that evolution had preserved favorable genetic variants and these had been made dominant as a way that protected the species from new mutations, which were largely held to be harmful. But if most mutations were recessive, if they rose in frequency eventually even random mating would generate recessive homozygote, and hence severely defective, offspring. We had adapted to the 'load' of mutations from these normal exposures, but could we adapt to a huge additional dose imposed by modern life? The survivors of Hiroshima and Nagasaki provided a kind of natural experiment to answer this question.
At the time it seemed that there was plenty to fear. The A-bombs were a lesson, but after the war, we had plenty of routine exposures: we had nuclear testing and the fear of the damage of fallout, which was wind-borne from test sites to much of the whole globe. There was growing diagnostic and therapeutic exposure to radiation. There were casual uses such as in shoe stores to see how things fit your feet (and kids like me played with them while our parents shopped for shoes). We were getting annual chest x-rays to look for tuberculosis, and dentists were firing away (I once had a job evaluating the degree of calibration of dentists' x-ray machines). Radiation was even a treatment for cancers that had arisen for other reasons.
Nuclear power stations had employees and the uranium that fueled them had to be mined, processed, and shipped. How much radiation could workers safely be exposed to? So questions about the nature of exposure were cogent at the time. Indeed, Neel's studies of the Yanomami and other Amazonian tribes, on the results of which I did some work early in my career, were in part designed to see what the genetic load was like in indigenous populations who where not exposed to these industrial-world dangers, to compare to what we found in ourselves.
In the first decades after the attacks studies of inherited mutation were first done using various traits like stillbirth as indicators and later a few protein polymorphisms were found that could be detected by electrophoresis during the decades after the attacks in those pregnant when exposed or in exposed survivors who hadn't been so disfigured or shunned that they were able to marry and have children whose DNA could be compared to their parents'. Essentially, very little if any excess mutation was found.
In a sense, this was presented as 'no mutations were found', a surprise given the expectations. However, what was instead clearly found rather quickly was that survivors were at greatly increased risk for cancer. First to appear clearly were leukemias, excess of which showed up in the first decade or so. Then excess cases of some solid tumors arose, with somewhat less risk and after longer latency times, and this excess continued throughout the survivors' lives.
The techniques for germ-line mutation detection were crude by today's standards, being based on protein electrophoresis and only for a limited number of genes, and for evidence of chromosomal anomalies, but I think the result still generally holds. After all, gonadal tissue is a small target relative to lungs and other organs, in terms of numbers of vulnerable dividing cells. And harmed gametes might just not have a chance to compete for fertilization and gestation.
But the cancer findings showed clear evidence of radiation as a mutagen, because cancers are to a fundamental extent diseases of genetic mutations that transform individual body cells so that they no longer behave as they should for their particular organ. They divide and spread. So cancer is a genetic disease, and radiation is a mutagen, and that's why it's also a carcinogen.
Findings like these for cancer fit into a cancer genetics research perspective, and with huge improvements in sequencing and genotyping technologies we gradually have grown to view genes as the major target for research into biological causation. Even in the Japanese survivors, however, an important fact is that except for leukemias, solid tumors didn't arise for many years after the bombings. This must reflect the fact that it takes many genetic changes to turn cells normal enough to enable gestation and postnatal life into tumor cells. The victims who experienced post-exposure cancers may have inherited some risk variants, but the latency time implies that they had to await some number of additional, non-radiation-related mutations to supplement those caused by the exposure, before a tumor arose.
Relevance to today's genetics
These things are relevant to the insistence today that genes are responsible for major diseases. For decades, starting with Archibald Garrod's pioneering use of Mendel's ideas to show that some metabolic diseases clustered among close relatives ('segregated') in the way Mendel's chosen pea traits did, human genetics was about clear-cut, basically single-gene pediatric traits. Indeed, Jim Neel related in his autobiography (Physician to the Gene Pool) that he was discouraged from doing genetics as a research clinician because there was nothing beyond rare pediatric traits to study.
It was a 1954 book by Neel and Schull, among a few others, that pioneered the idea that there might be genetic factors contributing to late-onset traits like cancer (not associated with radiation) and others, that aggregated but didn't segregate in families, that is, had weak effects (a point still not well-learned by today's army of geneticists). This foreshadowed the era of genetic epidemiology that has gradually led to the notion that your inherited genome is like your palm-lines in foretelling your life and fortunes. That genetic variation could 'cause' traits that take decades to develop was a strange thought, and we should recognize why we have such a trouble finding major factors for such complex, non-segregating late-onset diseases. The A-bomb studies found little detectable inherited mutation, including little or no new single-gene diseases, but showed clearly that somatic mutation was a result of the exposure of survivors (this was basically related to cancer as a trait, since there was then nothing in the way of specific responsible genes, since there was no way to identify them: they were assumed). That is one reason I've personally been interested in somatic mutation and its sources and consequences, and why I am skeptical about what I think are highly exaggerated notions about specific genetic causation of complex traits.
I can't judge Ham's book and its political or historical inferences. He asserts that the bombs were dropped perhaps needlessly for reasons of global politics involving competition among the winners for domination of Asia. Dropping the bomb let us get there first. However, for me, the book presents a disturbing, sad chronicle of what the survivors' experience, though it discusses the biomedical consequences rather scantly (it's mainly about the politics). It is easy to have great sympathy for the horrified, scarred, often shunned survivors of events the rest of the population would rather forget or pretend never happened. It is easy to criticize the political motivations made at the time, when fallible mortal leaders had to make judgment calls in a very complex political web with countless military and civilian people being horrified, mangled, or killed on a daily basis. Other nations on both sides were known to be working on a nuclear bomb. The Japanese were not innocent babes being unfairly punished, and they had committed unconscionable cruelty and horror on their enemies.
Of course, as always the ordinary citizen was caught up in global affairs beyond his or her control–as we are today. The lesson isn't to blame countries for their wartime atrocities, because no country is angelic under such stress. The lesson is to prevent such conflict in the first place. That seems to be a lesson nobody can learn, given what we see today, even in Europe and Asia, even among the WWII belligerents. We are prisoners of our emotions and our short memories.
But geopolitics aside, it is interesting to think about the ways that radiation mutagenesis and carcinogenesis have molded our thoughts more broadly, when it comes to the causes of death and disease even in ordinary times like ours.
Source: http://ecodevoevo.blogspot.com/2015/03/the-lucky-ones-were-vaporized-hiroshima.html
